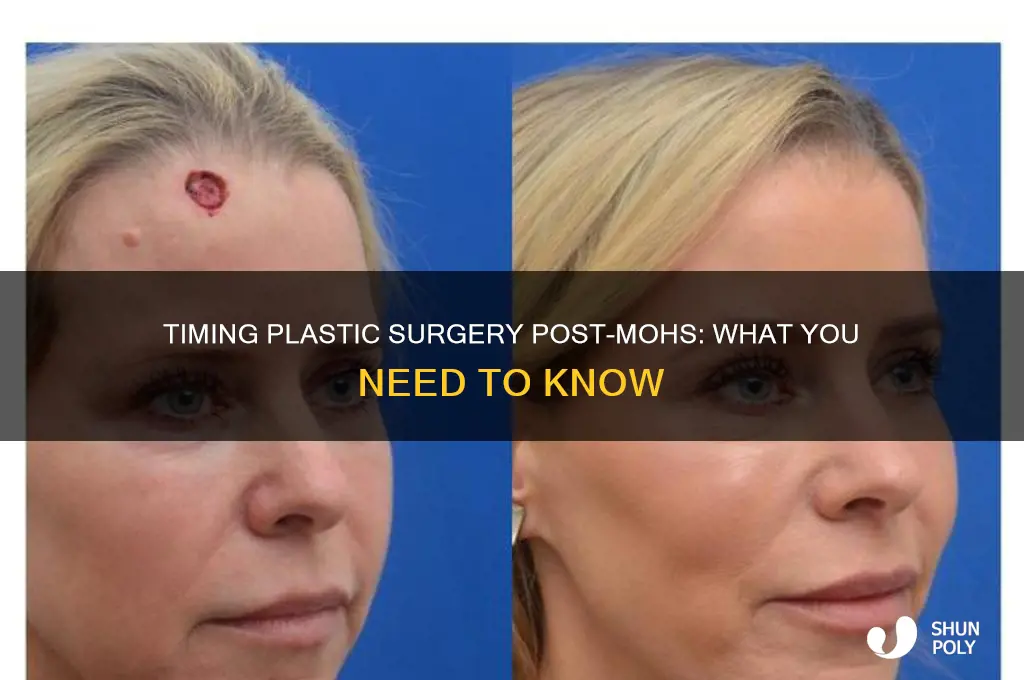
Following Mohs surgery, a precise technique used to remove skin cancer, patients often wonder about the timeline for undergoing plastic surgery to address any resulting scars or defects. Generally, the timing for plastic surgery depends on the extent of the Mohs procedure and the individual’s healing process. For minor cases, reconstructive surgery may be performed immediately after Mohs, while more complex or larger defects might require a waiting period of 2 to 6 weeks to ensure proper wound healing and reduce the risk of complications. It’s crucial to consult with both the Mohs surgeon and plastic surgeon to determine the optimal timing, as this ensures the best aesthetic and functional outcomes while minimizing potential risks.
Explore related products






What You'll Learn
- Timing for Revision Surgery: Ideal waiting period post-Mohs before plastic surgery intervention
- Healing Considerations: Factors affecting skin recovery and readiness for additional procedures
- Scar Assessment: When to evaluate Mohs scars for potential plastic surgery correction
- Surgeon Coordination: Importance of communication between Mohs and plastic surgeons for timing
- Patient Readiness: Physical and emotional preparedness for secondary plastic surgery post-Mohs
![]()
Timing for Revision Surgery: Ideal waiting period post-Mohs before plastic surgery intervention
The timing for revision surgery after Mohs micrographic surgery is a delicate balance between allowing the initial wound to heal and addressing cosmetic concerns promptly. Generally, surgeons recommend waiting 3 to 6 months before pursuing plastic surgery intervention. This window allows the skin to regain strength, reduce inflammation, and minimize the risk of complications like infection or poor wound healing. However, the exact timeline depends on factors such as the size and location of the Mohs defect, the patient’s overall health, and the type of reconstructive procedure planned. For instance, smaller defects on the forehead or cheek may heal sufficiently within 3 months, while larger or more complex areas, such as the nose or lips, might require closer to 6 months.
From an analytical perspective, the rationale behind this waiting period lies in the body’s natural healing process. Mohs surgery removes cancerous tissue layer by layer, often leaving a wound that needs time to stabilize. Premature intervention can disrupt collagen formation, impair blood flow, and compromise the structural integrity of the repair. Studies show that patients who wait the recommended period experience better cosmetic outcomes and fewer revisions. For example, a 2021 study in *Dermatologic Surgery* found that patients who underwent reconstruction after 4 months had a 25% lower revision rate compared to those who waited only 2 months. This data underscores the importance of patience in achieving optimal results.
Instructively, patients should follow a structured post-Mohs care routine to prepare for revision surgery. Keep the wound clean and moisturized, avoid sun exposure, and adhere to all post-operative instructions from the dermatologist. If stitches are involved, allow them to dissolve or be removed as scheduled. During the waiting period, consult with a plastic surgeon to discuss expectations and plan the procedure. For instance, if a skin graft or flap reconstruction is needed, the surgeon may recommend specific scar management techniques, such as silicone gel sheets or pressure garments, to optimize the donor site’s appearance.
Persuasively, rushing into plastic surgery after Mohs can lead to suboptimal outcomes and unnecessary complications. While the desire to restore appearance quickly is understandable, the body’s healing timeline cannot be accelerated without risk. For example, a patient who underwent nasal reconstruction just 6 weeks post-Mohs experienced wound dehiscence and required a second revision. Conversely, a patient who waited 5 months achieved a seamless result with minimal scarring. These contrasting cases highlight the value of adhering to the recommended waiting period.
Comparatively, the ideal timing for revision surgery differs from other post-surgical interventions. For instance, after a facelift or breast augmentation, patients typically wait only 2 to 3 weeks before resuming light activities. However, Mohs surgery involves the removal of cancerous tissue, which demands a more cautious approach. The skin’s integrity is compromised, and the body’s resources are focused on healing rather than recovery from elective procedures. This distinction emphasizes why the 3- to 6-month waiting period is non-negotiable for Mohs patients.
In conclusion, the ideal waiting period of 3 to 6 months post-Mohs before plastic surgery intervention is grounded in both scientific evidence and clinical experience. By allowing the skin to heal fully, patients can achieve better cosmetic results and reduce the likelihood of complications. Practical steps, such as diligent wound care and early consultation with a plastic surgeon, can further enhance outcomes. Patience, in this context, is not just a virtue—it’s a necessity for successful revision surgery.
Jessi's Transformation: Unveiling the Truth About Plastic Surgery Rumors
You may want to see also
Explore related products






![]()
Healing Considerations: Factors affecting skin recovery and readiness for additional procedures
The timing for additional procedures after Mohs surgery isn’t one-size-fits-all. Skin recovery varies based on factors like wound size, location, and individual healing rates. For instance, a small lesion on the forearm might heal within 2–3 weeks, while a larger defect on the face could take 6–8 weeks or longer. Understanding these variables is crucial for planning reconstructive surgery without compromising results.
Location matters significantly. High-tension areas like joints or the face heal slower due to increased movement and blood flow. For example, a wound near the mouth or nose may require 4–6 weeks of healing before plastic surgery, whereas a less mobile area like the calf might be ready in 3 weeks. Patients should avoid stretching or straining the surgical site during this period to prevent scarring or reopening.
Individual health plays a pivotal role. Smokers, diabetics, or those with compromised immune systems often experience delayed healing. Studies show smokers’ wounds take up to 50% longer to heal due to reduced oxygen delivery. Similarly, older adults (over 65) may require an additional 1–2 weeks for recovery. Adhering to post-operative care, such as keeping the area clean and applying prescribed ointments, accelerates healing and prepares the skin for further intervention.
Wound complexity dictates the timeline. Simple excisions heal faster than those requiring skin grafts or flaps. For instance, a grafted area needs 3–4 weeks for the donor and recipient sites to stabilize before considering additional procedures. Surgeons often recommend waiting until the wound is fully epithelialized (new skin formed) and any redness or swelling has subsided, typically 4–8 weeks post-Mohs.
Practical tips can expedite readiness. Elevating the surgical site, especially on the face, reduces swelling and promotes blood flow. Avoiding sun exposure prevents hyperpigmentation and irritation. Patients should follow a nutrient-rich diet (vitamins A, C, and zinc) to support collagen production. Regular follow-ups with the surgeon ensure the wound is healing optimally, allowing for a precise timeline for subsequent plastic surgery.
Ultimately, patience is key. Rushing into reconstructive procedures risks poor outcomes, such as widened scars or tissue breakdown. By respecting the body’s natural healing process and addressing individual factors, patients can achieve both functional and aesthetic success in their post-Mohs journey.
John Kerry's Appearance: Plastic Surgery Speculations and Facts Revealed
You may want to see also
Explore related products





![]()
Scar Assessment: When to evaluate Mohs scars for potential plastic surgery correction
Mohs surgery, a precise technique for removing skin cancer, often leaves scars that patients may wish to revise. The timing of scar assessment is critical, as premature evaluation can lead to inaccurate predictions of long-term appearance. Typically, scars mature over 6 to 12 months, during which they flatten, lighten, and blend into surrounding skin. Evaluating a Mohs scar before this period risks underestimating its natural improvement, potentially leading to unnecessary procedures. For optimal decision-making, wait at least 6 months post-surgery before considering plastic surgery correction.
During the initial 6 months, focus on scar management rather than assessment. Silicone-based gels, pressure garments, and sun protection can significantly improve scar appearance. For example, applying silicone gel twice daily for 12 weeks has been shown to reduce redness and thickness. Avoid aggressive treatments like laser therapy or excision during this phase, as they can disrupt the healing process. Instead, document the scar’s progress monthly with photographs to track changes objectively.
At the 6-month mark, a formal scar assessment should be conducted by a plastic surgeon or dermatologist. Key factors to evaluate include scar type (hypertrophic, atrophic, or keloid), location, and patient concerns. For instance, a raised hypertrophic scar on the face may benefit from steroid injections, while a depressed scar might require filler or surgical revision. Patient expectations must align with realistic outcomes; not all scars can be completely erased, but most can be significantly improved.
Beyond 6 months, reassessment at 12 months is advisable for scars that show minimal improvement. By this stage, the scar’s final appearance is more predictable, and advanced treatments like laser resurfacing or surgical excision can be planned. For example, fractional CO2 laser treatment, performed in 3 to 5 sessions spaced 4 weeks apart, can effectively smooth and blend scars. However, caution is warranted in areas prone to keloids, where surgical revision may exacerbate scarring.
In summary, scar assessment for potential plastic surgery correction should begin no earlier than 6 months after Mohs surgery, with a follow-up at 12 months if needed. Early management with proven techniques can enhance outcomes, while premature intervention risks complications. By adhering to this timeline, patients and providers can make informed decisions that balance aesthetic goals with surgical feasibility.
David Muir Plastic Surgery: Fact-Checking the Rumors and Speculations
You may want to see also
Explore related products

![The Natural Healing Handbook, Spiral-Bound Guide for Herbal Remedies and Natural Recipes, by Ancient Remedies. [Spiral-bound] Ancient Remedies (The ... Remedies) [Spiral-bound] Ancient Remedies](https://m.media-amazon.com/images/I/81Nbi516Z3L._AC_UL320_.jpg)


![First Honey Wound Healing Ointment [ 1oz - 28.4g ] | 100% Active Leptospermum | Fast Relief & Skin Repair | Manuka Honey from New Zealand | Antibiotic Free Burn Care, Scar Gel, Dressing Aid](https://m.media-amazon.com/images/I/71UM74F73hL._AC_UL320_.jpg)
![]()
Surgeon Coordination: Importance of communication between Mohs and plastic surgeons for timing
Effective coordination between Mohs surgeons and plastic surgeons hinges on precise communication regarding timing, as this directly impacts wound healing, cosmetic outcomes, and patient satisfaction. Mohs surgery, a precise technique for removing skin cancer, often leaves defects requiring immediate or delayed reconstruction. The plastic surgeon’s involvement must align with the Mohs surgeon’s assessment of tissue viability, wound size, and patient-specific factors like comorbidities or medication use. For instance, a small defect on the cheek may allow for same-day reconstruction, while a large nasal defect might necessitate a 1-2 week delay to optimize blood flow to the area. Without clear communication, misalignment in timing can lead to complications such as poor wound closure or compromised aesthetic results.
A structured protocol for surgeon coordination can streamline this process. Mohs surgeons should provide plastic surgeons with detailed information post-excision, including defect size, depth, and location, as well as any intraoperative challenges encountered. Plastic surgeons, in turn, must communicate their preferred timing for reconstruction based on the planned technique—whether direct closure, skin grafting, or flap reconstruction. For example, a forehead flap for nasal reconstruction typically requires a 3-week delay to ensure pedicle vascularization, whereas a full-thickness skin graft might proceed within 48 hours. Establishing a shared checklist or digital communication platform can reduce errors and ensure both parties are aligned on the timeline.
Patient education is another critical aspect of this coordination. Patients often underestimate the complexity of post-Mohs reconstruction and may pressure surgeons to expedite the process. Clear, unified messaging from both surgeons about the rationale behind the chosen timeline—whether immediate or delayed—can manage expectations and foster trust. For instance, explaining that delaying reconstruction for a complex ear defect reduces the risk of necrosis can help patients understand the benefits of patience. Providing written post-operative instructions and follow-up schedules further reinforces this collaborative approach.
Finally, the financial and logistical implications of timing cannot be overlooked. Insurance coverage for staged procedures varies, and delays in reconstruction may require additional pre-authorizations or documentation. Surgeons must coordinate not only clinically but also administratively to avoid billing disputes or coverage denials. For example, coding a nasal reconstruction as a staged procedure rather than a single event can prevent reimbursement issues. By integrating clinical, patient-centered, and administrative considerations, effective surgeon coordination ensures optimal outcomes while minimizing stress for both patients and providers.
Did Donnie Swaggart Undergo Plastic Surgery? Unveiling the Truth
You may want to see also
Explore related products






![]()
Patient Readiness: Physical and emotional preparedness for secondary plastic surgery post-Mohs
The timing for secondary plastic surgery after Mohs surgery isn’t one-size-fits-all. While some sources suggest waiting 3–6 months for optimal wound healing, others emphasize the importance of individual patient factors. For instance, a 55-year-old patient with a large defect on the nose might require a longer healing period compared to a 30-year-old with a smaller lesion on the forearm. The key lies in assessing both physical and emotional readiness, as rushing into reconstructive surgery can compromise results and increase complications.
Physically, the Mohs wound must reach a stable state before plastic surgery can proceed. This involves monitoring for signs of infection, ensuring proper scar maturation, and confirming that the skin graft or flap (if previously applied) has fully integrated. For example, a patient who underwent Mohs on the cheek might need to wait until the initial redness and swelling subside, typically around 8–12 weeks. During this period, adhering to post-Mohs care instructions—such as avoiding sun exposure, keeping the area clean, and using prescribed topical medications—is critical. Skipping these steps can delay healing and jeopardize the success of subsequent plastic surgery.
Emotionally, patients must navigate the psychological impact of both the cancer diagnosis and the visible changes to their appearance. A study published in *JAMA Dermatology* found that 40% of Mohs patients experience anxiety or depression post-procedure, particularly if the surgery leaves a noticeable scar. Before proceeding with plastic surgery, patients should feel confident in their decision, understanding that reconstruction aims to improve function and aesthetics but may not restore the area to its pre-cancer state. Support from a counselor or support group can be invaluable during this phase, helping patients process their emotions and set realistic expectations.
A practical approach to assessing readiness involves a three-step evaluation: 1. Physical Examination by the dermatologist or plastic surgeon to confirm the wound is fully healed; 2. Emotional Check-In with the patient to gauge their mental state and readiness for another procedure; and 3. Discussion of Goals to align expectations with achievable outcomes. For example, a patient seeking rhinoplasty after Mohs on the nose should understand that the focus will be on restoring symmetry and function, not achieving perfection. This structured approach ensures that both patient and surgeon are on the same page, reducing the risk of dissatisfaction post-reconstruction.
Ultimately, patient readiness is a dynamic process that requires patience, communication, and collaboration. While the physical timeline might suggest waiting 3–6 months, emotional preparedness can take longer. By prioritizing both aspects, patients can approach secondary plastic surgery with confidence, knowing they’ve given their body and mind the time needed to heal. This holistic approach not only enhances surgical outcomes but also fosters a smoother recovery and greater satisfaction with the final results.
Al Pacino's Transformation: Plastic Surgery Rumors and Reality Revealed
You may want to see also
Frequently asked questions
Typically, plastic surgery can be performed immediately after Mohs surgery, often in the same surgical session, depending on the complexity of the defect and the surgeon’s expertise.
Yes, it’s safe to wait, but delaying plastic surgery may affect the cosmetic outcome, as scar tissue can form and make reconstruction more challenging.
Plastic surgery is generally performed once the Mohs wound is clean and free of infection, but minor procedures can sometimes be done before complete healing if the surgeon deems it appropriate.
Waiting too long can lead to suboptimal cosmetic results, as the skin may lose elasticity or scar tissue may form, making reconstruction more difficult.
Combining the procedures is generally safe when performed by experienced surgeons, but there may be increased risks of infection, bleeding, or prolonged recovery time.