Plastic surgery during World War I underwent a transformative evolution, driven by the unprecedented scale of facial and bodily injuries sustained by soldiers on the front lines. The war’s brutal trench warfare and advancements in weaponry, such as shrapnel and high-velocity bullets, resulted in severe disfigurements, particularly to the face and limbs. Surgeons like Harold Gillies pioneered innovative techniques to reconstruct these injuries, laying the foundation for modern plastic surgery. Gillies, often regarded as the father of plastic surgery, developed methods like skin grafting and tissue transfer to restore function and appearance to wounded soldiers. This period marked a shift from purely functional repairs to a focus on both physical and psychological rehabilitation, as surgeons sought to help survivors reintegrate into society with dignity. The war’s legacy in plastic surgery not only advanced medical techniques but also highlighted the profound human cost of conflict.
| Characteristics | Values |
|---|---|
| Purpose | Reconstruction of facial and bodily injuries sustained by soldiers, primarily due to gunshot wounds, shrapnel, and burns. |
| Key Figure | Sir Harold Gillies, a New Zealand-born surgeon, is considered the father of modern plastic surgery for his pioneering work during WW1. |
| Techniques | Skin grafting, bone and tissue reconstruction, and the "tubed pedicle" technique to transfer skin from one part of the body to another. |
| Location | Aldershot, England, where Gillies established the first dedicated plastic surgery unit in 1915. |
| Patients | Primarily soldiers with severe facial injuries, often referred to as "broken faces" or "baskets cases." |
| Success Rate | Varied, but many patients experienced significant improvements in appearance and function, though complete restoration was rare. |
| Anesthesia | Local and general anesthesia were used, with techniques evolving during the war to improve safety and efficacy. |
| Post-Op Care | Extensive, including bandaging, splinting, and physical therapy to aid healing and restore function. |
| Psychological Impact | Plastic surgery provided not only physical restoration but also psychological relief, helping soldiers reintegrate into society. |
| Legacy | Laid the foundation for modern plastic and reconstructive surgery, influencing techniques and principles still used today. |
Explore related products






What You'll Learn
- Facial Reconstruction Techniques: Pioneering skin grafts, bone realignment, and tissue repair for war-injured soldiers
- Harold Gillies' Innovations: Development of modern plastic surgery by treating facial trauma patients
- Masks for Disfigurement: Custom-made prosthetics to restore appearance and confidence post-injury
- Psychological Impact: Addressing mental health through improved physical appearance after severe wounds
- Advancements in Anesthesia: Safer surgeries enabled by improved pain management techniques during procedures
![]()
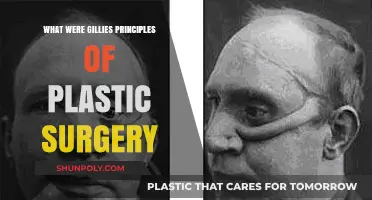
Facial Reconstruction Techniques: Pioneering skin grafts, bone realignment, and tissue repair for war-injured soldiers
The First World War's brutal trench warfare inflicted devastating facial injuries on soldiers, often leaving them disfigured and struggling with basic functions like breathing, eating, and speaking. This crisis spurred unprecedented advancements in facial reconstruction techniques, transforming plastic surgery from a niche practice into a vital medical discipline.
At the forefront of this revolution were skin grafts, a technique refined by pioneers like Harold Gillies. Gillies, a New Zealand-born surgeon, established a dedicated facial injury ward in Aldershot, England, where he developed methods for transferring healthy skin from one part of the body to the face. This involved carefully excising a thin layer of skin, often from the chest or buttocks, and suturing it onto the damaged area. The success of these grafts relied on meticulous planning, ensuring adequate blood supply to the transplanted tissue. Gillies' work not only restored physical appearance but also significantly improved patients' quality of life, allowing them to reintegrate into society with greater confidence.
Bone realignment was another crucial aspect of facial reconstruction during WWI. The war's high-velocity bullets and shrapnel caused complex fractures, often resulting in misaligned facial bones. Surgeons like Gillies and his colleague, Henry Tonks, an artist turned anatomist, developed innovative techniques to realign these bones using wire, plates, and screws. This meticulous process required a deep understanding of facial anatomy and artistic skill to restore symmetry and functionality. Tonks' artistic background proved invaluable, as he could visualize the desired outcome and guide the surgical reconstruction with precision.
These pioneering efforts laid the foundation for modern maxillofacial surgery, demonstrating the power of interdisciplinary collaboration between medicine and art.
Tissue repair, particularly for soft tissue defects, posed another significant challenge. Surgeons experimented with various techniques, including local flaps, where adjacent tissue was mobilized to cover the defect, and tubed pedicle grafts, where a tube of skin was created and tunneled under healthy tissue to reach the wound site. These methods required careful planning and patience, as the tissue needed time to heal and adapt to its new location. The development of these techniques not only addressed the immediate needs of war-injured soldiers but also established principles that continue to guide plastic surgery today.
The legacy of WWI facial reconstruction extends far beyond the battlefield. The techniques developed during this period revolutionized the field of plastic surgery, offering hope and restoration to patients with congenital deformities, trauma victims, and those seeking cosmetic enhancements. The war's tragic circumstances catalyzed medical innovation, leaving an indelible mark on the history of medicine and forever changing the way we approach facial reconstruction.
Jeff Dunham's Transformation: Plastic Surgery Rumors Explored and Debunked
You may want to see also
Explore related products






![]()
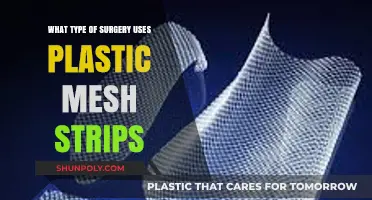
Harold Gillies' Innovations: Development of modern plastic surgery by treating facial trauma patients
The First World War brought an unprecedented scale of facial injuries, with soldiers enduring shrapnel wounds, gunshot injuries, and burns that left them disfigured. Amid this crisis, Harold Gillies emerged as a pioneer, transforming plastic surgery from a niche practice into a vital medical discipline. His work at the Cambridge Military Hospital in Aldershot, England, laid the foundation for modern reconstructive techniques, offering hope and restoration to those whose faces bore the brutal marks of war.
Gillies’ innovations began with a simple yet revolutionary approach: treating facial injuries as both functional and aesthetic challenges. He developed the "tubed pedicle" technique, a method of transferring skin from one part of the body to the face while maintaining its blood supply. This breakthrough allowed for larger grafts and reduced the risk of tissue death, a common issue in earlier attempts. For instance, a soldier with a severely damaged cheek could receive a skin graft from his chest, carefully shaped and sutured to restore contour and function. Gillies’ meticulous planning and execution ensured that each procedure was tailored to the patient’s unique injury, setting a standard for personalized care in plastic surgery.
Beyond surgical techniques, Gillies pioneered psychological support for patients, recognizing the emotional toll of facial disfigurement. He established a ward where patients could recover together, fostering a sense of community and mutual encouragement. This holistic approach was radical for its time, as medical care then focused primarily on physical survival. Gillies’ wards became spaces of healing, where soldiers learned to adapt to their new appearances and rebuild their lives. His emphasis on psychological well-being remains a cornerstone of modern reconstructive surgery, reminding practitioners that restoring a patient’s self-esteem is as crucial as repairing their body.
Gillies’ legacy extends to his training of other surgeons, ensuring his methods would outlast the war. He mentored pioneers like Archibald McIndoe, who later applied these techniques to treat burn victims in the Second World War. Gillies’ detailed documentation of cases, including before-and-after photographs and surgical diagrams, created a knowledge base that continues to educate surgeons today. His work not only saved lives but also redefined the possibilities of medical innovation under extreme circumstances, proving that even in the darkest times, humanity can advance through compassion and ingenuity.
Legal Age for Plastic Surgery: Must You Wait Until 18?
You may want to see also
Explore related products






![]()
Masks for Disfigurement: Custom-made prosthetics to restore appearance and confidence post-injury
The First World War left an indelible mark on the faces and minds of those who fought, with disfiguring injuries becoming a grim hallmark of trench warfare. For soldiers whose faces bore the brunt of shrapnel, bullets, or burns, the physical and psychological scars ran deep. Enter the pioneering work of surgeons like Harold Gillies, who transformed plastic surgery from a niche practice into a lifeline for the disfigured. Among their most innovative solutions were custom-made prosthetics, often referred to as "masks," designed to restore not just appearance but also the shattered confidence of those who wore them.
Crafting these masks was an art as much as a science. Each prosthetic was tailored to the individual, beginning with detailed measurements and molds of the patient’s face. Materials ranged from lightweight metals to early plastics like celluloid, chosen for their durability and ability to mimic skin tone. Painters and sculptors were often enlisted to add lifelike details—eyebrows, facial hair, even freckles—ensuring the mask blended seamlessly with the wearer’s features. For instance, a soldier missing his nose might receive a prosthetic attached with adhesive or a discreet harness, allowing him to re-enter society without drawing unwanted stares.
The psychological impact of these masks cannot be overstated. For men who had once felt condemned to a life of isolation or ridicule, these prosthetics offered a chance to reclaim their identities. One notable example is the "Tin Noses Club," a support group for soldiers with facial injuries, many of whom relied on such devices. The club’s motto, "We bear our scars with pride," underscores the dual purpose of these masks: to heal the visible wounds of war while fostering a sense of camaraderie among those who wore them.
Yet, the process was not without challenges. Early prosthetics were often uncomfortable, prone to slipping, or difficult to maintain. Wearers had to learn how to clean and adjust their masks daily, a task that required patience and practice. Moreover, the materials available at the time were far from perfect; celluloid, for instance, could warp in heat or cold, while metal prosthetics were heavy and prone to corrosion. Despite these limitations, the masks represented a monumental leap forward in both medical and emotional rehabilitation.
Today, the legacy of these custom-made prosthetics endures in modern facial reconstruction techniques. While materials and methods have advanced dramatically, the core principle remains the same: to restore not just the face, but the spirit of those who have endured unimaginable trauma. For the soldiers of World War I, these masks were more than mere devices—they were symbols of resilience, ingenuity, and the unyielding human desire to rebuild, both inside and out.
Erin Napier Plastic Surgery: Fact-Checking the Home Town Star's Look
You may want to see also
Explore related products





![]()
Psychological Impact: Addressing mental health through improved physical appearance after severe wounds
World War I saw an unprecedented surge in facial injuries, with explosives and trench warfare leaving thousands of soldiers disfigured. Plastic surgery, still in its infancy, became a critical tool not only for physical reconstruction but also for psychological rehabilitation. Surgeons like Harold Gillies pioneered techniques to repair shattered jaws, noses, and eyes, often using skin grafts and bone restructuring. However, the focus wasn’t merely on restoring function; it was equally about restoring identity and self-worth. For soldiers returning home, a recognizable face was as vital as a working limb, as it directly impacted their ability to reintegrate into society and rebuild their lives.
Consider the case of a 24-year-old soldier who suffered a gunshot wound to the face, leaving him with a missing cheekbone and a collapsed eye socket. After multiple surgeries, including a bone graft from his hip and a skin graft from his thigh, his facial structure was partially restored. While the physical transformation was remarkable, the psychological shift was even more profound. Pre-surgery, he avoided mirrors and social interactions, plagued by feelings of shame and isolation. Post-surgery, he reported a renewed sense of confidence, even returning to his pre-war profession as a teacher. This example underscores how addressing physical disfigurement can be a cornerstone of mental health recovery, offering a tangible way to combat trauma and stigma.
The process of psychological healing through plastic surgery wasn’t linear. Patients often underwent dozens of procedures over years, each step fraught with uncertainty and pain. Surgeons had to manage expectations, emphasizing gradual improvement rather than instant perfection. For instance, a soldier with severe burns might require 10–15 surgeries spaced months apart, each focusing on a specific area like the lips, eyelids, or ears. During this time, psychological support was crucial. Many hospitals integrated counseling and peer support groups, recognizing that mental resilience was as important as physical endurance. This holistic approach laid the groundwork for modern multidisciplinary care in reconstructive surgery.
Critics might argue that focusing on appearance perpetuates superficial values, but in the context of wartime trauma, it’s a practical and compassionate intervention. A study from the 1920s noted that soldiers who received facial reconstruction were 40% more likely to maintain employment and 60% less likely to report symptoms of depression compared to those left untreated. This data highlights the tangible societal benefits of such procedures. For survivors, a restored face wasn’t about vanity—it was about reclaiming agency in a world that often judged them harshly for their injuries.
In practice, modern clinicians can draw lessons from this era. For patients with severe wounds, whether from combat, accidents, or illness, combining reconstructive surgery with mental health support is essential. Start by setting realistic goals, both physical and emotional, and involve psychologists early in the treatment plan. Encourage patients to document their progress through journals or photographs, as visual evidence of improvement can be a powerful motivator. Finally, foster a community of survivors, as shared experiences can reduce feelings of isolation and foster hope. By addressing both the face and the mind, we honor the legacy of WWI plastic surgery and its profound impact on human resilience.
Sarah Jessica Parker's Transformation: Plastic Surgery Rumors Explored
You may want to see also
Explore related products





![]()
Advancements in Anesthesia: Safer surgeries enabled by improved pain management techniques during procedures
World War I marked a pivotal era in medical history, particularly in the realm of plastic surgery, where the sheer scale of injuries demanded unprecedented innovation. Amidst the chaos, one of the most critical advancements was in anesthesia—a field that transformed surgeries from harrowing ordeals into more manageable procedures. Before the war, anesthesia was rudimentary, often limited to ether or chloroform administered without precise control. The war’s demands spurred the development of safer, more effective pain management techniques, laying the groundwork for modern surgical practice.
Consider the introduction of nitrous oxide and the refinement of ether administration. Surgeons began using a mixture of nitrous oxide and oxygen, known as "laughing gas," to induce a state of relaxation and pain relief. Ether, while effective, was volatile and required careful handling to avoid complications like respiratory depression. Innovations like the Boyle’s machine, a precursor to modern anesthesia machines, allowed for controlled delivery of gases, reducing the risk of overdose. These advancements were not just theoretical; they were battlefield necessities, enabling surgeons to perform lengthy reconstructive procedures on soldiers with facial injuries, gunshot wounds, and burns.
The role of anesthetists became increasingly specialized during this period. Prior to the war, anesthesia was often administered by nurses or junior doctors with minimal training. By 1917, dedicated anesthesia teams emerged, trained to monitor patients’ vital signs and adjust dosages in real time. This shift was critical in reducing mortality rates during surgery. For instance, the use of rectal thermometers and blood pressure cuffs became standard practice, allowing anesthetists to detect early signs of shock or hypoxia. Such monitoring techniques were rudimentary by today’s standards but revolutionary at the time.
A key takeaway from this era is the importance of dosage precision. Ether, for example, required careful titration—typically starting at 5-10% concentration and adjusted based on the patient’s response. Overdosing could lead to cardiac arrest, while underdosing left patients in agony. The war forced medical professionals to refine these techniques, often through trial and error. By its end, anesthesia had evolved from a risky necessity to a cornerstone of surgical safety, enabling plastic surgeons to undertake complex procedures with greater confidence.
Practically, these advancements had long-term implications beyond the battlefield. They underscored the need for interdisciplinary collaboration in medicine, as surgeons, anesthetists, and nurses worked together to improve patient outcomes. For modern practitioners, the lessons are clear: pain management is not just about alleviating discomfort but about creating conditions for successful surgery and recovery. Whether in reconstructive surgery or routine procedures, the principles of safe anesthesia developed during WWI remain foundational, a testament to the ingenuity born of necessity.
Madison Beer Plastic Surgery: Fact-Checking Rumors and Speculations
You may want to see also
Frequently asked questions
Plastic surgery during World War I primarily focused on reconstructing facial and bodily injuries sustained by soldiers, particularly those caused by shrapnel, bullets, and chemical weapons. It aimed to restore function and appearance, improving soldiers' quality of life.
Key figures included Harold Gillies, a New Zealand-born surgeon who established the first dedicated plastic surgery unit in Aldershot, England, and Hippolyte Morestin, a French surgeon who advanced techniques for facial reconstruction. Their work laid the foundation for modern plastic surgery.
Surgeons employed techniques such as skin grafting, tissue transfer, and bone restructuring. They also developed methods like the "tubed pedicle" technique, which allowed for the gradual movement of skin flaps to cover large wounds, minimizing scarring and improving healing.